

ACL Rupture: Surgery Vs Non-Surgical Management

The ACL is one of the ligaments that connect the femur to the tibia at the knee joint.
ACL ruptures most commonly occur in young and active individuals that participate in sports such as basketball, rugby, soccer, netball etc. Approximately 30% of ACL injuries occur via contact mechanisms, with 70% via non-contact mechanisms.
ACL ruptures often occur with associated injuries such as medial collateral ligament (MCL) and meniscus tears (prevalence of 30% and 45% respectively), whilst the rates of associated posterior cruciate ligament (PCL) and lateral collateral ligament (LCL) injuries are generally low.

Grades of ACL sprains
Grade 1 sprain is the least severe ACL injury. This means that the ACL is stretched but is still intact. The ACL is still capable of keeping the knee joint stable
Grade 2 - a partial ligament tear. This means that the ACL is stretched, and is loose.
Grade 3 sprain is a complete tear of the ACL and is the most common type of ACL sprain.
More common: Non- contact ACL tear
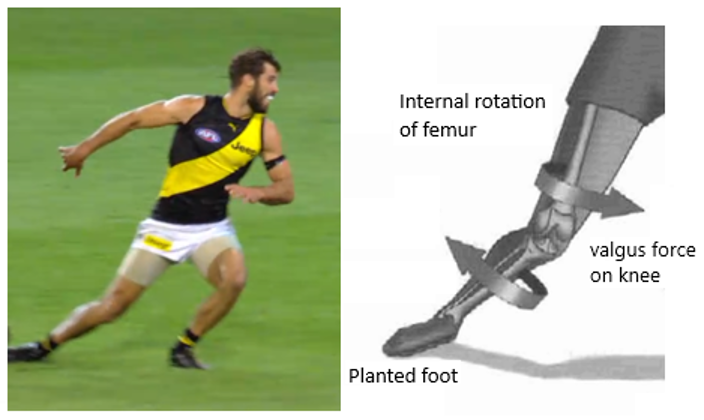
The athlete is often distracted, they’re looking at whats coming next, they’re watching the players that they’re uncoordinated to defend against or attack. Or it can be uncoordinated jump landing, the foot is planted on the ground and the femor rotates on the planted tibia, that torque exceeds the tensile strength of the ACL and it ruptures
Mechanism of injury
Injury mechanism that involves acceleration/deceleration in combination with a knee valgus load (refer to pic above)
Side stepping
Cutting actions, pivoting (Uncoordinated sidestep)
Direct trauma to the knee
Leading to a dynamic valgus mechanism -> failure of ACL = popping sensation in the knee

Less common: Contact ACL Tear
Symptoms of ACL tear
An audible “pop” may be heard or a snapping sensation could be felt in your knee.
Knee pain and swelling
Loss of range of motion
Instability of the knee (knee feels like its locking, catching, giving away during movement)
Discomfort when walking
Tenderness along the line of the joint
Surgery Vs Non-Surgical Management
Non-Surgical - Cross Bracing Protocol
(Named after Dr. Mervyn Cross: one of the pioneer surgeons of ACL surgery, and Sports and Exercise Physician Dr Tom Cross)
New and exciting evidence has continued to support the fact that certain ACL ruptures can be healed with natural healing. The new piece of research is called the cross bracing protocol. 80 patients with confirmed ACL rupture (10-58 years old) participated in the trial conducted by Dr Stephanie Filbay (Senior Research Associate in the Department of Physiotherapy at the University of Melbourne).
For the protocol:
The patient will put on a knee brace that is locked at 90 degrees for 4 weeks. This is because the 2 torn ends of the ACL are in the closest proximity at 90 deg flexion. And holding that in position in a knee brace was hypothesized to facilitate healing.
The range of motion of the brace will be increased weekly with full knee range of motion achieved in 10 weeks and brace removed at 12 weeks. This is combined with physio supervised exercise based rehab, whilst the brace is on and whilst the brace is off.
At 3 months, 72/80(90%) of the participants had evidence of ACL healing on MRI. (Grade 1 heal at 3 months reported better healing compared with grade 2 or fully ruptured at 12 months follow up.)
At 6 months follow up, already 6 patients progressed from grade 1 to grade 0 ACL.
With the Cross bracing protocol 62% of participants return to pre-injury sport VS post ACL surgery an average of 55% return to sport.
What does this show? It shows that conservative treatment for the ACL can stand its ground when compared to surgery. Why does this matter? Keep on reading.

Another trial (KANON) compared participants randomized to rehabilitation or optional delayed ACL reconstruction (ACLR).
16 out of 54 (30%) rehab-only participants displayed evidence of ACL healing on MRI (grade 0) at 2- year follow-up.
58% (95% CI 39 to 76%) of 24 rehab-only participants had evidence of ACL healing on MRI at 5-year follow-up.
It was found that there was no difference in the results of surgery or rehab-only at 2 and 5 years follow up.
Again, why is there so much research on conservative care?
It’s because ACL surgery has been shown to cause a lot of trauma to the knee joint.
It’s quite naive to think that a graft from the hamstring or patella can behave like the native ACL which has its own proprioceptive fibres, vascularisation, pain fibres and a quite complex anatomy.
Surgery
If you’re thinking about opting for surgery, here are some quick facts beforehand.
ACL Reconstruction FAQs
Does early ACL reconstructions lead to better patient outcomes? No
Are ACL reconstructions necessary to return to sport? No
Do ACL reconstructions reduce the chance of osteoarthritis? No, on the contrary, it increase the chances of radiological osteoarthritis by 3 times (radiological doesn’t necessarily mean symptomatic)
Do ACL reconstructions prevent further knee damage? No, unless presented with persistent functional instability, then surgery would prevent knee damage.
Can some ACL tears heal naturally? Yes
Do you need an expert surgeon for ACL surgeries for some but not all ACL ruptures? Absolutely
Can Physios help with ACL healing?
The answer is yes! Whether you opt for conservative treatment or decide to go for surgery (which I would only advise to do only if conservative treatment fails), physios can help with reducing pain & swelling, regaining strength & mobility, and returning to your desired activities.
Exercises prescribed by your physio will be aimed to strengthen the muscles that support the knee. Especially the upper leg muscles (quadriceps and hamstrings). The 3 main factors we will try to restore are:
Range of motion
Strength
Stability
This is purely from a mechanical standpoint. If you’re looking to return to sports, your physio will work together with you and your coach to guide you through a safe and effective return to sports plan.
When should you start physio after an ACL tear?
Conservative:
Immediately after injury.
Post-Op:
First week post-operation, the goal is to regain range of motion by commencing gentle exercises, especially at knee extension. The aim for exercise is to increase blood flow and to reduce swelling.
If there was no meniscus repair, you can bear weight immediately after surgery. For the first 2 months, a range of motion of 120-140 degrees knee flexion is a good target.
Surgery or no surgery, as swelling subsides, you will start your rehab program.
Specific exercises will be introduced by your physio to reduce pain & swelling and to restore movement in knee and increase knee strength
Requires commitment to long term program to guide through every phase of rehab, and progress you through various stages as you improves
Final thoughts on ACL
ACLs injuries are common in the setting of sports especially in the younger population.
You might be able to function normally without an ACL.
The average cost of an ACL reconstruction is 7.5-15k AUD with a re-rupture rate of ~6%.
With or without surgery, your knee function will be the same at around 2-5 years post injury.
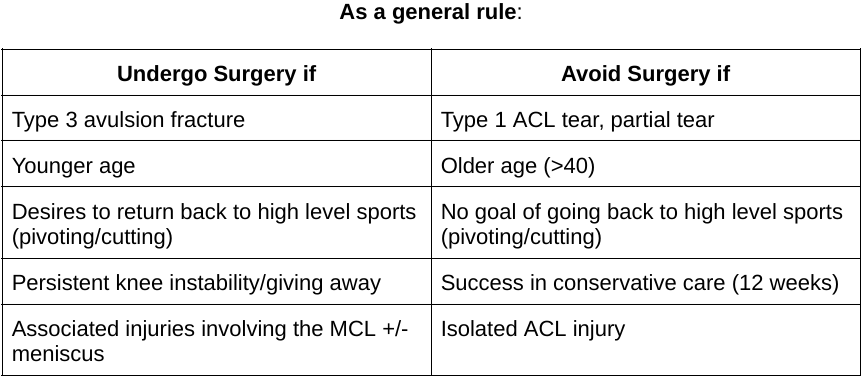
Surgery can be considered for:
Young athletes that wish to return to high level sports (cutting/pivoting)
Or with people that have persistent instability that have failed conservative rehab at least 12 weeks.
The cross bracing protocol is new evidence that reinforces conservative treatment. Patients that are suitable for the protocol will be managed by a physio and also an orthopaedic surgeon.
The Important consideration is that you can try conservative treatment first and then go for surgery if conservative doesn't work. However, once you decide to get surgery, you would have missed your chance of trying non-operative care.
Physios are trained to aid with the healing of ACL injuries and are movement specialists who help people through hands-on care, education, along with prescribed exercise and movements.
Unsure if you have an ACL injury or how to manage a knee injury? Book Now to arrange an appointment.
Hope this helps.
Your friendly neighborhood physio,
Tony.
Resources
Barenius, B., Ponzer, S., Shalabi, A., Bujak, R., Norlen, L., Eriksson, K. (2014). Increased risk of osteoarthritis after anterior cruiciate ligament reconstruction: a 14-year follow-up study of a randomized controlled trial Retrieved from: https://pubmed.ncbi.nlm.nih.gov/24644301/
Crawford, S., Lubowitz, B. (2013). Long-term failure of anterior cruciate ligament reconstruction
Retrieved from: https://pubmed.ncbi.nlm.nih.gov/23820260/
Filbay, S., Ackerman, I., Russell, T., Crossley, K. (2016). Return to sports matters-longer-term quality of life after ACL reconstruction in people with knee difficulties
Retrieved from: https://pubmed.ncbi.nlm.nih.gov/27167588/
Filbay, S., Dowsett, M., Jomaa, M., Rooney, J., Sabharwal, R., Lucas, P., Heever, A., Kazaglis, J., Merlino, J., Moran, M., Allwright, M., Kuah, D., Durie, R., Roger, G., Cross, M., Cross, T. (2023). Healing of acute anterior cruciate ligament rupture on MRI and outcomes following non-surgical management with the Cross Bracing Protocol.
Retrieved from: https://bjsm.bmj.com/content/early/2023/06/13/bjsports-2023-106931
Filbay, S., Grindem, H. (2019). Evidence-based recommendations for the management of anterior cruciate ligament (ACL) rupture
Retrieved from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6723618/
Filbay, S., Roemer., Lohmander, L., Turkiewicz, A., Roos, E., Frobell, R., Englund, M. (2023). Evidence of ACL healing on MRI following ACL rupture treated with rehabilitation alone may be associated with better patient-reported outcomes: a secondary analysis from the KANON trial.
Retrieved from: https://bjsm.bmj.com/content/57/2/91
Fleming, J., Ritzmann, R., Centner, C. (2022). Effect of an Anterior Cruciate Ligament Rupture on Knee Proprioception Within 2 Years After Conservative and Operative Treatment: A Systematic Review with Meta-Analysis
Retrieved from: https://link.springer.com/article/10.1007/s40279-021-01600-z